Prader-Willi Syndrome Drug Market Heats Up: 5 Upcoming Challengers to Soleno’s VYKAT XR
May 27, 2026
Since the FDA approved recombinant human growth hormone (rhGH) for Prader-Willi syndrome (PWS) in 2000, several companies have encountered difficulties in developing more effective therapies for hyperphagia, the persistent and uncontrollable hunger associated with the disorder. However, in March 2025, Soleno Therapeutics marked a major milestone with the approval of VYKAT XR (diazoxide choline), making it the first FDA-approved Prader-Willi syndrome drug for hyperphagia. VYKAT XR is indicated for patients aged 4 years and older with PWS, a disorder characterized by low muscle tone, short stature, and cognitive and developmental difficulties.
Before that, multiple companies have encountered obstacles in their efforts to develop treatments for hyperphagia in Prader-Willi syndrome. In 2016, Alize Pharma achieved positive results in a Phase II trial with AZP-531, a first-in-class unacylated ghrelin peptide analog, but was unable to advance the treatment further. That same year, Zafgen demonstrated beloranib’s efficacy, a MetAP2 inhibitor, in a Phase III trial, but safety concerns ultimately led to its discontinuation. Saniona developed Tesomet, a combination of the monoamine reuptake inhibitor tesofensine and the beta blocker metoprolol. Although Tesomet received an Orphan Drug designation from the FDA in 2021, its development was discontinued in 2022 due to funding constraints.
Gedeon Richter also evaluated RGH-706 for hyperphagia associated with PWS; however, based on preliminary Phase II data, the company decided not to pursue further development of the molecule for this indication.
Downloads
Click Here To Get the Article in PDF

Recent Articles
- Advances in Prader-Willi Syndrome Treatment: New Hope for Patients
- Neurocrine Signs Deal to Acquire Soleno Therapeutics; AstraZeneca Shares Favorable Results from E...
- Gilead’s Magrolimab Plus Azacitidine for MDS; FDA Approveds VANFLYTA for Newly Diagnosed AML; FDA...
- Cellenkos’ CK0801 Granted FDA Orphan Drug Status for Aplastic Anemia; Mirum’s LIVMARLI Gets FDA N...
Meanwhile, Acadia Pharmaceuticals pursued intranasal carbetocin, but the FDA rejected the treatment in 2022. Acadia had previously acquired the candidate through a USD 10 million purchase of Levo Therapeutics. After this, in 2025, Acadia reported that the Phase III COMPASS PWS trial failed to demonstrate statistically significant improvement over placebo on the primary hyperphagia endpoint or any secondary endpoints. Following these disappointing topline results, the company announced that it would discontinue further development of intranasal carbetocin for PWS.
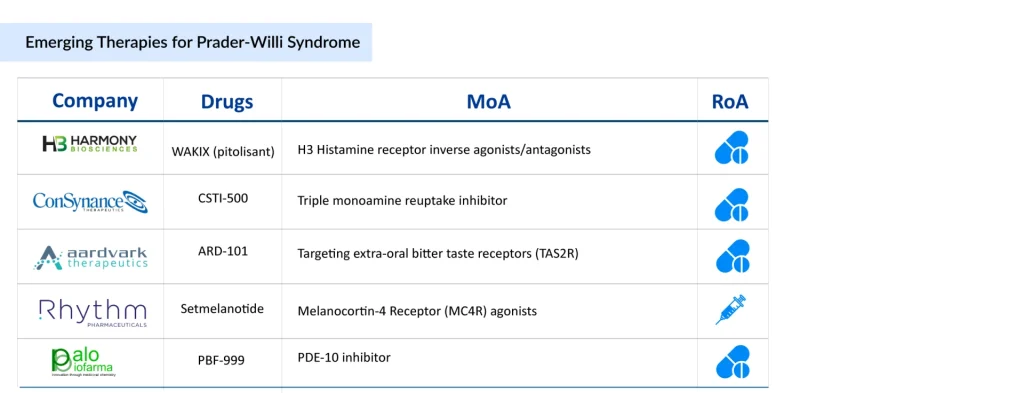
Several Prader-Willi syndrome drugs are currently in mid and late-stage development, with potential approvals on the horizon. The evolving treatment landscape includes a diverse array of therapeutic options, such as H3 histamine receptor inverse agonists/antagonists (WAKIX [pitolisant]), therapies targeting extra-oral bitter taste receptors (TAS2R) (ARD-101), PDE-10 inhibitors (PBF-999), triple monoamine reuptake inhibitors (CSTI-500), melanocortin-4 receptor agonists (Setmelanotide), among others.
Let’s take an in-depth review of these upcoming Prader-Willi syndrome drugs and how they will challenge Soleno’s recently approved VYKAT XR.
Harmony Biosciences’s WAKIX
WAKIX (pitolisant) is a selective histamine 3 (H₃) receptor antagonist/inverse agonist. While its exact mechanism of action remains unclear, its effectiveness is believed to stem from its interaction with H₃ receptors, leading to increased histamine synthesis and release, a key neurotransmitter involved in wakefulness.
Developed by Bioprojet (France), Harmony Biosciences holds the exclusive US rights to develop, manufacture, and commercialize pitolisant. WAKIX is FDA-approved for the treatment of excessive daytime sleepiness or cataplexy in adult patients with narcolepsy and for the treatment of EDS in pediatric patients 6 years of age and older with narcolepsy, but it is not yet approved for Prader-Willi syndrome and remains under evaluation for this condition. In February 2024, the FDA granted Orphan Drug Designation (ODD) to pitolisant for PWS treatment.
Pitolisant in PWS is currently advancing through late-stage development, with Phase III topline data readout expected in 2H 2026. Currently, WAKIX is the only therapy being studied for PWS patients with EDS, which affects approximately 50% of PWS patients. Given the high unmet medical need, limited competition, and established efficacy in narcolepsy, WAKIX is expected to gain strong commercial traction and have an extended market uptake period if approved for PWS.
Aardvark Therapeutics’ ARD-101
Aardvark’s lead candidate, oral ARD-101, is a potent pan-agonist of bitter taste receptors (TAS2R) that stimulates enteroendocrine cells in the digestive tract, triggering the release of gut-peptide hormones like GLP-1 and cholecystokinin (CCK), a satiety hormone that activates gut-brain signaling to regulate hunger. ARD-101 has demonstrated hunger reduction both as a monotherapy and in combination with existing GLP-1 therapies.
Based on encouraging clinical data from its ongoing trial, the FDA has granted ARD-101 both Orphan Drug Designation and Rare Pediatric Disease Designation for Prader-Willi syndrome. In March 2026, Aardvark Therapeutics announced that the US FDA had placed a full clinical hold on its investigational new drug application for ARD-101 related to the Company’s previously announced voluntary pause. The clinical hold applies to all ongoing clinical studies under the IND, including the Phase III HERO trial (AVK-101-301) evaluating ARD-101 for the treatment of hyperphagia in patients with PWS. The Company remains in active discussions with the FDA to support resolution of the clinical hold. In parallel with its ongoing engagement with the FDA, Aardvark intends to unblind the clinical data accumulated to date across the HERO trial to assess the totality of available efficacy and safety data and to support an informed determination of next steps for the ARD-101 program.
Palobiofarma’s PBF-999
PBF-999 is an innovative PDE10 inhibitor developed by Palobiofarma, which has shown potent and selective inhibition of the PDE10 enzyme in preclinical studies. PDE10 plays a crucial role in regulating cyclic nucleotide levels, which are key signaling molecules in the brain. A Phase II PWS clinical trial evaluating PBF-999 is currently ongoing. PBF-999 has already undergone three clinical studies, where an appetite-suppressing effect was observed. Based on these findings, Palobiofarma has designed a new clinical trial to evaluate the safety and efficacy of PBF-999 in reducing hyperphagia in adults with PWS.
In March 2024, Pamplona announced that both the FDA and EMA had granted ODD to PBF-999 for treating PWS. Additionally, in November 2023, Palobiofarma received a Rare Pediatric Disease Designation (RPDD) from the US FDA for PBF-999 in PWS treatment.
The company recently achieved two major milestones, including the successful completion of a Phase II clinical trial in 32 patients aged 12 years and older, which demonstrated a clinically meaningful reduction in hyperphagia along with a favourable safety and tolerability profile. In addition, Palobiofarma completed successful End-of-Phase II meetings with both the FDA and EMA, receiving regulatory feedback on critical components of the Phase III development program and paving the way for advancement toward late-stage development. The company remains committed to initiating the pivotal Phase III study in early 2027.
ConSynance Therapeutics’s CSTI-500
CSTI-500 is a triple monoamine reuptake inhibitor (TRI) that modulates serotonin, dopamine, and norepinephrine by inhibiting their respective transporters (SERT, DAT, and NET). These neurotransmitters are key regulators of behavior, feeding, and mood control. CSTI-500 is an innovative, orally administered New Chemical Entity (NCE) designed to restore key neurotransmitter balance in PWS.
In April 2026, The Foundation for Prader-Willi Research (FPWR) announced a venture philanthropy investment in ConSynance Therapeutics to support the advancement of CSTI-500, ConSynance’ s investigational therapy for the treatment of behavioral dysregulation and hyperphagia in PWS. The investment will support a Phase IIa clinical study of CSTI-500 in individuals with PWS, expected to begin in 2026.
Rhythm Pharmaceuticals’ Setmelanotide
Setmelanotide, an Melanocortin-4 Receptor (MC4R) agonists designed to treat hyperphagia and severe obesity, is approved by the US FDA to reduce excess body weight and maintain weight reduction long term in adult and pediatric patients 2 years of age and older with syndromic or monogenic obesity due to Bardet-Biedl syndrome (BBS) or genetically confirmed pro-opiomelanocortin (POMC), including proprotein convertase subtilisin/kexin type 1 (PCSK1), deficiency or leptin receptor (LEPR) deficiency. It is currently being investigated in a Phase II clinical trial for patients with PWS.
In December 2025, Rhythm Pharmaceuticals announced positive preliminary results from its exploratory Phase II trial of setmelanotide in patients with PWS. The Company also announced plans to advance setmelanotide into a Phase III registrational trial in PWS, pending successful completion of this Phase II trial. Rhythm also announced that it has initiated a Part D arm in the Phase I trial of MC4R agonist RM-718 that will enroll up to 20 patients with PWS. Rhythm anticipates screening the first patient for this 26-week open-label trial of RM-718 in December 2025.
The anticipated launch of emerging therapies in the Prader-Willi syndrome landscape is expected to reshape the competitive dynamics, posing both challenges and opportunities for Soleno’s VYKAT XR. The introduction of new therapies—particularly those with novel mechanisms of action or broader symptom coverage—may fragment prescriber preferences and intensify competition for patient share. This could pressure VYKAT XR’s pricing flexibility, market uptake, or label expansion strategies, particularly if newer entrants demonstrate superior efficacy, safety, or convenience.
On the flip side, the entry of additional therapies may also help validate the commercial viability of the PWS space, attracting greater attention from payers, clinicians, and advocacy groups. If VYKAT XR maintains a first-to-market or best-in-class status, it can leverage early relationships with key stakeholders and real-world data to defend and expand its market position.
Furthermore, Soleno’s accumulated experience in navigating the unique regulatory and access challenges in PWS may offer a strategic edge over newer players. Ultimately, the evolving competitive landscape will require Soleno to invest in post-marketing evidence, targeted physician engagement, and differentiation strategies to retain leadership in this rare but high-need therapeutic area.

FAQs
Because the biology of hyperphagia in PWS is extremely complex, multiple pathways (ghrelin, oxytocin, MCH, histamine) influence appetite. Most earlier drugs targeted a single pathway and ran into safety or efficacy hurdles.
Yes. Some of these candidates target sleep disorders, behavioral regulation, or gut–brain signaling, which means they may end up addressing multiple symptoms of PWS beyond appetite.
These incentives are crucial because PWS is a rare disease with high development risk. Without FDA’s ODD or RPDD benefits, most companies couldn’t justify the enormous R&D costs.
Surprisingly, yes. Some PWS trials are testing combinations with GLP-1s to enhance satiety. If successful, it could blur the line between mainstream metabolic drugs and rare-disease therapies.
More competitors validate the market, attract payer attention, and increase advocacy momentum. Sometimes the first-to-market drug benefits the most because it’s already embedded in treatment protocols.
Because PWS primarily affects the brain, intranasal delivery provides a shortcut to the central nervous system while reducing systemic exposure and side effects.
Absolutely. Mechanisms like TAS2R activation, PDE-10 inhibition, or MCHR1 blockade could inspire obesity treatments for much larger populations if they prove safe and effective in PWS.
Downloads
Article in PDF
Recent Articles
- Neurocrine Signs Deal to Acquire Soleno Therapeutics; AstraZeneca Shares Favorable Results from E...
- Advances in Prader-Willi Syndrome Treatment: New Hope for Patients
- Gilead’s Magrolimab Plus Azacitidine for MDS; FDA Approveds VANFLYTA for Newly Diagnosed AML; FDA...
- Cellenkos’ CK0801 Granted FDA Orphan Drug Status for Aplastic Anemia; Mirum’s LIVMARLI Gets FDA N...



